APEX PWR | Physical Therapy Feature
Cleared by Your Surgeon Doesn't Mean Cleared for Sport
- Surgeon clearance confirms structural healing of the graft and basic range of motion. It does not confirm the limb can absorb force, decelerate, or hold up under fatigue.
- Returning to cutting and pivoting sports before 9 months after ACL reconstruction increases reinjury risk by a factor of more than 4 (Grindem et al., 2016).
- Athletes who passed all return-to-sport criteria had a reinjury rate of 5.6 percent versus 38.2 percent in those who failed any criteria, an 84 percent reduction.
- In athletes under 25 who return to cutting sports, the second ACL injury rate is approximately 23 percent, or roughly 1 in 4 (Wiggins et al., 2016).
- Objective testing should include strength symmetry, hop testing, deceleration and change-of-direction performance, sprint speed, and psychological readiness.
If you or your athlete recently had knee surgery and the surgeon said the words "you're cleared," it's tempting to treat that as the finish line. The stitches are out, the swelling is down, range of motion looks good. Sport is calling. Practice starts Tuesday.
That moment is one of the highest risk windows in the entire recovery process. Surgeon clearance confirms that the surgical work has healed. It does not confirm that the knee, the leg, or the athlete is ready to handle the forces of sport. The data on what happens when athletes treat the two as the same is sobering, and it has been replicated across enough peer-reviewed cohorts that it is no longer up for serious debate.
A surgeon's job is to make sure the ACL healed. A physical therapist's job is to make sure the athlete can handle sport again. Those are two different finish lines, and the gap between them is where re-injuries happen.
"Clearance by time, simple visual, and hands-on tests cannot accurately quantify the readiness of your limb. Deficits in power production and single-leg jumping control are evident in athletes who return to sport without fully completing rehab. Reinjury risks in ACL patients are still way too high, often from premature clearance and not fully dotting your I's and crossing your T's objectively."
Dr. Jon van den Boogaard, DPT, OCS · Director of Rehab, APEX PWR
What Surgeon Clearance Actually Tests For
Orthopedic surgeons are skilled at what they do. They take care of the surgical side of recovery. When they clear a patient at six months, they are confirming a specific set of things, and they are doing it with the diagnostic tools that fall within their scope of practice.
What surgeon clearance confirms
- The graft or repair has structurally healed and integrated
- Range of motion has returned to functional levels
- There are no signs of infection, hardware complications, or surgical failure
- Basic strength has returned to a baseline level
- Imaging and clinical exam show stable structural integrity
What surgeon clearance does not test
- Force absorption during landing from a jump or cut
- Deceleration mechanics at speed
- Change-of-direction performance under fatigue
- Power output relative to the uninvolved limb
- Reactive control in unpredictable, sport-like environments
- Psychological readiness to plant, cut, and trust the knee under pressure
None of that is a knock on surgeons. It's a recognition that sport readiness lives in a different scope. Testing for those qualities, and training the athlete back to the point of passing those tests, is the work of the rehab and performance team.
The Research on Premature Return
Two studies form the backbone of how serious clinicians think about this question. They are both worth knowing by name if you or your athlete are post-op.
The first is the Delaware-Oslo ACL Cohort Study, published by Grindem and colleagues in the British Journal of Sports Medicine in 2016. They followed 106 athletes who underwent ACL reconstruction and tracked their return-to-sport timing, the testing they did or didn't pass, and their reinjury rates over two years. The findings were striking: patients who returned to level I sports (cutting, pivoting, jumping) had a 4.32 times higher reinjury rate than those who did not. More importantly, the reinjury rate was significantly reduced by 51 percent for each month return to sport was delayed until 9 months after surgery, after which no further risk reduction was observed. And the headline number: 38.2 percent of athletes who failed RTS criteria suffered reinjuries, versus 5.6 percent of those who passed. That is an 84 percent reduction in reinjury risk from one variable: passing objective return-to-sport testing.
The second is the systematic review and meta-analysis by Wiggins and colleagues in the American Journal of Sports Medicine, also in 2016, which pooled data from 23,740 patients. The total second ACL reinjury rate across the population was 15 percent. In patients younger than 25 who returned to sport, it climbed to 23 percent. As the authors put it: nearly 1 in 4 young athletic patients who sustain an ACL injury and return to high-risk sport will go on to sustain another ACL injury at some point in their career, and they will likely sustain it early in the return-to-play period.
These two studies, viewed together, point to a clear conclusion: the timeline matters, the testing matters, and the two combined produce dramatically better outcomes than either one alone.
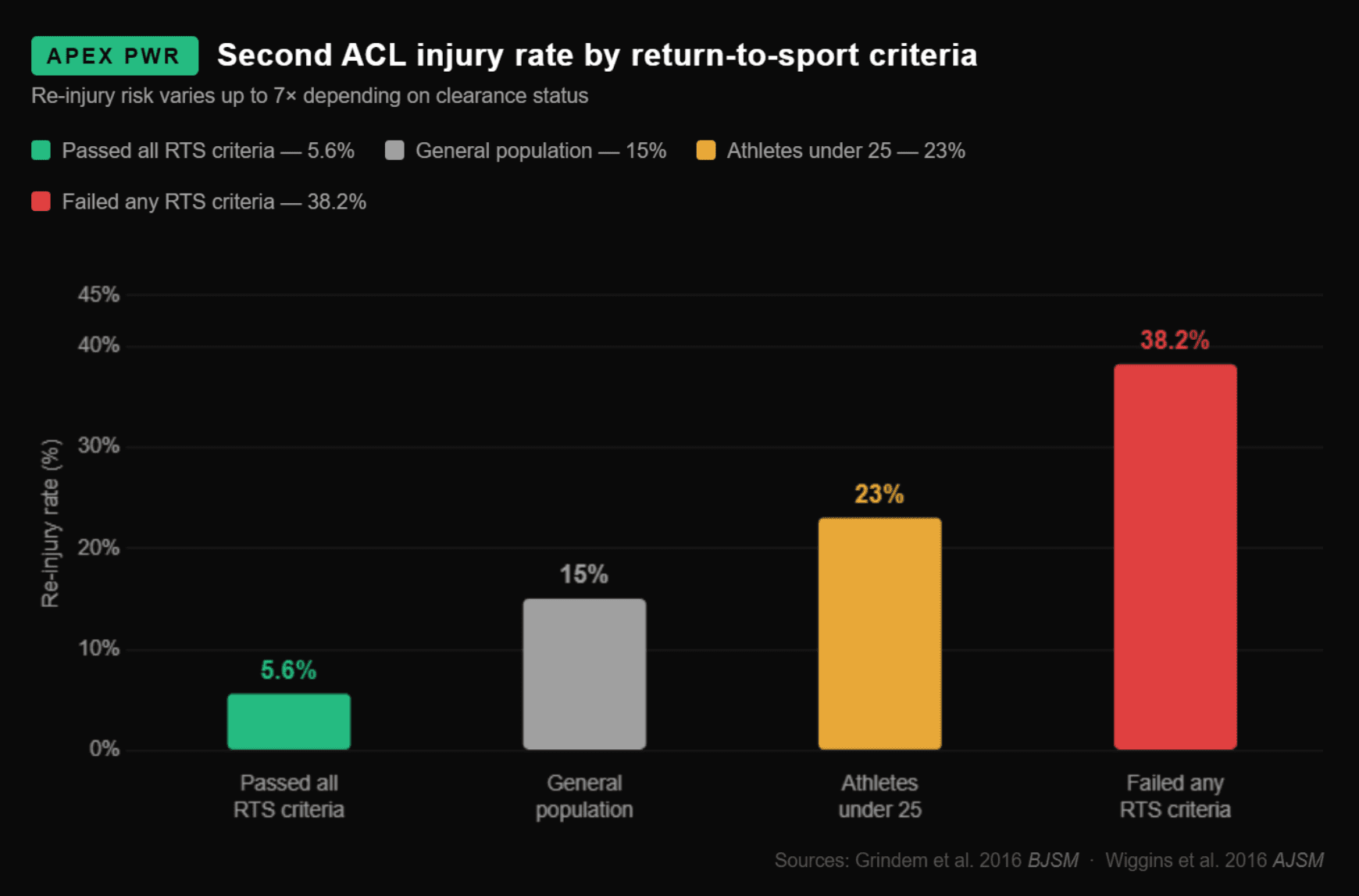
Reinjury rates vary by an order of magnitude depending on whether athletes pass objective return-to-sport testing. Data: Grindem et al. (2016) BJSM & Wiggins et al. (2016) AJSM.
The APEX Knee Rehab Progression
At APEX, our post-op knee work is structured in four stages. The stages are not strict time blocks. They are performance gates. An athlete progresses to the next stage when they hit the objective criteria, not when the calendar says so.
Restore
The early stage. Restore range of motion, normalize gait, eliminate effusion, rebuild quadriceps activation, and re-establish neuromuscular signaling. This is where we partner most closely with the surgeon's protocol and protect the healing graft. The goal here is foundational, not flashy.
Reinforce
Build foundational bilateral and unilateral strength. The non-operative limb often loses strength too during this phase, so symmetry is a moving target. We use isometric and progressive resistance work, eccentric loading, and targeted single-leg progressions. By the end of this stage, an athlete should be tolerating significant external load through full ranges, with strength symmetry trending toward parity.
Reactivate
Reintroduce plyometrics, deceleration, landing mechanics, change of direction, and reactive control. This is the stage that surgeon clearance does not test for, and it is the stage that closes the gap between "the knee is healed" and "the athlete can absorb force at speed." Stage 3 work is high-skill, deliberate, and built on top of the strength foundation from stage 2.
Return
Full sport-specific demands, tested under fatigue, against objective benchmarks. Sprint speed measured with timing gates. Hop performance compared limb-to-limb. Strength and power symmetry confirmed with dynamometry. Psychological readiness assessed with validated tools. The athlete graduates to sport with evidence, not a vibe.
What This Looks Like on the Floor
Below are short clips from active cases at APEX. Different athletes, different stages, different surgeries. Each one shows the kind of work that lives beyond surgeon clearance.
Dr. Dustin Zink, DPT, working with an athlete 7 months post-op ACL reconstruction.
Dr. Zink with a different athlete 6 months post-op ACL reconstruction.
Torque-to-bodyweight ratio testing on a post-op meniscus patient. Why we measure it, and what it tells us.
Speed training and VALD speed gate testing with a post-op ACL athlete in the final stages of return-to-sport.
The work shown above happens in the same building as the strength training floor, which matters. An athlete in stage 3 of knee rehab does not need to drive to a separate gym to start running, jumping, and cutting under coaching. The progression is continuous.
The Testing We Use
Objective testing is the bridge between rehab and sport. We use a combination of tools chosen for their reliability and their relevance to the demands of cutting, jumping, and pivoting sports.
- Force plates and dynamometry for quadriceps and hamstring strength symmetry, peak torque relative to bodyweight, and rate of force development.
- Single-leg hop testing (four variations: single hop, triple hop, crossover hop, timed hop), with a Limb Symmetry Index target above 90 percent on each test.
- VALD speed gates for sprint timing across 10, 20, and 30 meter splits, with limb-by-limb deceleration patterns assessed where possible.
- Plyometric and landing mechanics screening for drop landings, lateral hops, and reactive ground contacts.
- Change-of-direction testing (505 test, T-test, or sport-specific variations) under fatigue.
- Validated psychological readiness questionnaires such as the ACL-RSI (Return to Sport after Injury) scale.
No single test makes the call. The full battery is the call. An athlete who has 95 percent quad strength symmetry but lands asymmetrically and reports low confidence in the knee is not ready, even if one number looks good in isolation.
Why This Matters Beyond the Athlete
A second ACL tear is not just another nine to twelve months of rehab. It carries a meaningfully higher risk of cartilage damage, a higher risk of post-traumatic osteoarthritis years later, and significantly worse psychological outcomes around return to sport. The decision to skip the gap between surgeon clearance and full sport readiness is the kind of decision that can echo across the next thirty years of someone's knee.
For parents of youth athletes, this matters even more. Younger athletes have the highest reinjury rates, the highest activity demands, and the longest time horizon for the consequences of a second tear. The Wiggins data on 23 percent reinjury in under-25s returning to sport is most acute in 14- to 22-year-olds.
How Patients Start With Our PT Team
The most complete version of this work happens when we have a patient from the start. We can protect the surgical site in the early weeks, build strength on a predictable timeline, and own the return-to-sport testing at the end. When that path is available, that is what we recommend.
It is not the only path. We regularly bring on athletes and active adults at mid- and late-stages, including:
- Patients partway through PT elsewhere who want to keep progressing
- Athletes who were recently cleared by their surgeon and are not ready to stop training
- Patients who have used up their insurance visits or authorization but still have work to do
- Athletes who finished a full course of PT and want a return-to-sport battery before going back to play
For these cases, the most common formats are self-pay one-on-one physical therapy sessions, semi-private small group strength training, or a combination of both. A common pattern: a patient with a low insurance visit cap spaces out their covered PT sessions over a longer time horizon and fills in the gaps with three or four strength training sessions per week with a coach who knows their case. That cadence is difficult to match in a traditional PT clinic, and the consistency is part of what closes the gap between clearance and sport.
If you are not sure where you fit, the fastest path is to fill out the intake form on our physical therapy page. That is where every conversation starts.
Start the Conversation
Whether you're pre-op, recently post-op, mid-rehab elsewhere, or already cleared and looking for the next step, our team can map out a plan that fits your case. Fill out the form on our physical therapy page to get started.
Get StartedCommon Knee Surgeries We Rehabilitate
- ACL reconstruction (patellar tendon, hamstring, and quadriceps tendon grafts)
- Meniscus repair and partial meniscectomy
- MCL repair and reconstruction
- Patellar dislocation surgical repair (MPFL reconstruction)
- Multi-ligament knee reconstruction
- Cartilage repair procedures (microfracture, OATS, MACI)
Frequently Asked Questions
What does it mean when your surgeon clears you after knee surgery?
Surgeon clearance after knee surgery confirms that the surgical site has healed structurally: the graft has incorporated, basic range of motion has returned, and there are no signs of infection or hardware failure. It does not confirm that the limb can absorb force, decelerate at speed, tolerate fatigue, or perform the cutting and landing demands of sport. Sport readiness requires objective testing of strength symmetry, hop performance, power output, and psychological readiness, which falls within the physical therapy and performance rehab scope.
How long is rehab after ACL surgery before returning to sport?
Research from the Delaware-Oslo ACL Cohort Study demonstrates that returning to sport before 9 months post-surgery substantially increases reinjury rates, and that each month of delay until 9 months reduces reinjury risk by approximately 51 percent. Most athletes need a minimum of 9 to 12 months of structured rehabilitation before safely returning to cutting and pivoting sports, and clearance should be based on objective performance testing rather than time alone.
What is the second ACL injury rate after surgery?
A systematic review of 23,740 patients reported a second ACL injury rate of 15 percent across all patients and 23 percent in athletes under age 25 who returned to cutting and pivoting sports. Athletes who passed all return-to-sport criteria had a reinjury rate of 5.6 percent, compared to 38.2 percent in athletes who failed any criteria. That is an 84 percent reduction in reinjury risk from objective testing alone.
What testing should I complete before returning to sport after ACL surgery?
A complete return-to-sport battery should include quadriceps and hamstring strength symmetry testing, single-leg hop testing across four hop variations, plyometric and landing mechanics assessment, change-of-direction and deceleration testing, sprint speed measurement with timing gates, and a validated psychological readiness questionnaire such as the ACL-RSI. A Limb Symmetry Index above 90 percent on most measures is a common threshold, though current research suggests stricter thresholds may be appropriate for high-level athletes.
Where can I find post-op knee physical therapy near Portland, Oregon?
APEX PWR provides post-operative knee rehabilitation in Tigard, Oregon, serving the greater Portland metro area, including Beaverton, Lake Oswego, Tualatin, and Sherwood. Our physical therapy team includes board-certified orthopaedic specialists and sport-trained DPTs who work alongside performance coaches in the same facility, allowing for a continuous progression from early rehab through sport-specific return-to-play testing.
Can I start at APEX if I'm already partway through rehab elsewhere or have run out of insurance visits?
Yes. We take patients at every stage. The ideal scenario is starting with us from the beginning so we can build the full progression, but we regularly take on athletes who have already started PT elsewhere, who have been cleared by their surgeon and want to keep progressing, or who have exhausted their insurance visit cap. Mid- and late-stage cases typically work with us through self-pay one-on-one physical therapy sessions, semi-private small group strength training, or a combination of both. A common pattern for patients with limited insurance is spacing covered PT sessions over a longer time horizon while training three to four times per week with a strength coach who knows the case.
The Bottom Line
Surgeons heal the structure. Physical therapists, working alongside performance coaches and objective testing, prepare the athlete for the demands they're actually returning to. The data is clear that closing that gap matters. An athlete who passes a complete return-to-sport battery has roughly a 5 to 6 percent chance of reinjury. An athlete who skips that step and returns based on time and surgeon clearance alone is looking at a number closer to 23 to 38 percent.
If you or your athlete are post-op and the surgeon recently said the word "cleared," the next step is testing, not a return to play. Whether you start with us from day one, transition in mid-rehab, or come to us after insurance runs out, the path forward is the same: confirm the limb is ready with objective data, then graduate to sport on evidence rather than calendar time. Our intake form on the physical therapy page is the fastest way to start that conversation.
The APEX Team
Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. "Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study." British Journal of Sports Medicine, 2016;50(13):804-808. PMID: 27162233. DOI: 10.1136/bjsports-2016-096031.
Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. "Risk of Secondary Injury in Younger Athletes After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis." American Journal of Sports Medicine, 2016;44(7):1861-1876. PMID: 26772611.
Ardern CL, Taylor NF, Feller JA, Webster KE. "Fifty-five percent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors." British Journal of Sports Medicine, 2014;48(21):1543-1552.
Webster KE, Hewett TE. "Meta-analysis of Meta-analyses of Anterior Cruciate Ligament Injury Reduction Training Programs." Journal of Orthopaedic Research, 2018.
Journal of Orthopaedic & Sports Physical Therapy. "Better Safe Than Sorry? A Systematic Review with Meta-analysis on Time to Return to Sport After ACL Reconstruction as a Risk Factor for Second ACL Injury." JOSPT, 2023.